

Available at Royal Glenora, St. Albert, Windermere, Old Strathcona, and Capilano Rehabilitation Centre locations.
life doesn’t have to be dizzy
Leading Edge Physiotherapy is pleased to offer vestibular rehabilitation for those patients suffering from balance disorders and dizziness in Edmonton and St. Albert.
Bam… Out of nowhere a person can often be confronted by the scary feeling of not knowing what is happening in their head. Their world is literally turned upside down. Beyond disconcerting, this unusual feeling can also impact our lives in a massive way.
Simple activities like getting a haircut, rolling over in bed and going to yoga wreck havoc on their brain and its ability to sort out the world. It can lead to many outward consequences from nausea and vomiting to falling over.
Dizziness is one of the more common complaints among clients that enter the typical medical clinic. It often proves difficult to determine a diagnosis and appropriate treatment plan. This is not surprising given the time required to tease out the true nature of these symptoms and to conduct the differential diagnosis given the multitude of potential sources associated with dizziness. The result is that a large number of these cases are referred on to specialists like Otolaryngologists and Neurologists to review and manage. These referrals can often result in a diagnosis of one of a variety of peripheral or central vestibular conditions that do not require additional surgical or medical management.
Conditions such as vestibular neuronitis, labyrinthitis, and benign paroxysmal positional vertigo (BPPV) are the more common diagnoses that may fall into this category.
the Leading Edge approach:
In the cases of BPPV we use a very mechanical approach to examination and treatment that has been found to be exceptionally effective in resolution of the associated signs and symptoms. Most professionals are familiar with the typical Hallpike-Dix test and Epley maneuvers that are often associated with the management of these conditions. However, there are potentially 12 different presentations of BPPV. As much as the above approach is effective for the more common forms of BPPV, different techniques are often necessary for management of the other presentations. These are often the cases that sound like a BPPV but do not present with positive Hallpike-Dix tests or seem resistant to the typical treatment approach. Our therapists have specialized training and experience in identifying and effectively managing these exceptional cases, as well as the more common ones, using a variety of techniques and technology.
In those cases that involve an insult to the peripheral apparatus or nerve we take a very different but also very safe and effective approach to examination and treatment. A large number of these clients do find spontaneous recovery following an insult to the peripheral vestibular apparatus with effective central compensation. There are, however, a large number that require specific additional training to assist this process. Treatment is then tailored to the specific deficits identified on examination and is primarily exercise based with a focus on developing central compensation and optimizing the effects of neuroplasticity. This can often include dysfunctions of sensory organization, vestibulo-ocular reflex gain, static and dynamic postural stability, and motion sensitivity, among others.
Our first priority in the examination is the screening of vascular and neurological structures as well as conditions potentially requiring immediate medical attention. Our comprehensive assessment includes procedures designed to evaluate vestibulo-ocular (ear/eye) function, dynamic visual acuity (movement of the body or head and visual response), cervical spine biomechanics and kinesthetic function, sensory organization, static and dynamic postural stability, motion sensitivity, and various forms of nystagmus associated with specific conditions.
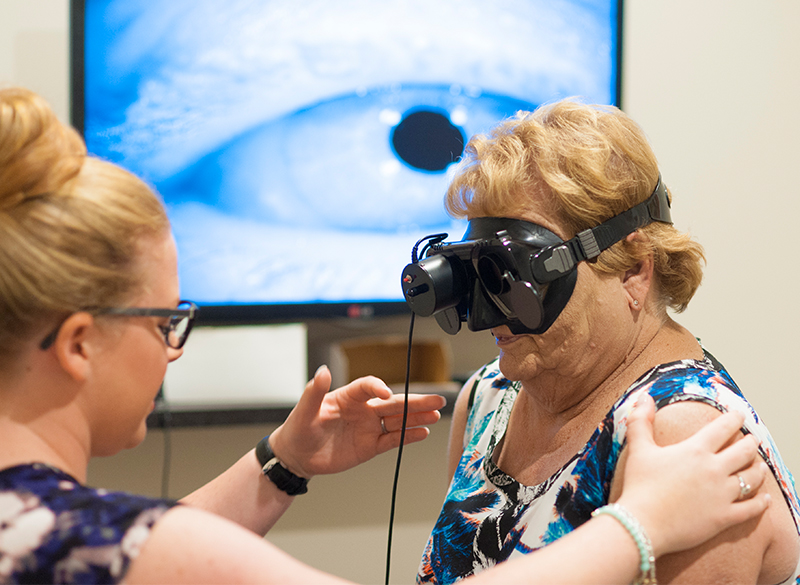
At Leading Edge, we use state-of-the-art infrared camera technology and visual suppression in blackout goggles to allow visualization of many specific forms of nystagmus that are not evident in room light testing. This technology is only utilized by a select few providers.

Vestibular disorders are problems that occur in the part of the inner ear responsible for position and motion sense of our body and head. When there is an issue with this system one of the most common symptoms that people experience is a sense of motion when they are not actually moving. The feeling of movement when you are stationary or continued movement when you have stopped moving is referred to as “vertigo”.
Our specially trained therapists can successfully help you manage:
- Benign Paroxysmal Positional Vertigo
- Unilateral Vestibular Hypofunction (Vestibular Neuritis, Labyrinthitis, Acoustic Neuroma, Vascular Compromise, Trauma)
- Bilateral Vestibular Hypofunction (Ototoxicity, Bilateral Endolymphatic Hydrops, Age related degeneration)
- Central Vestibular Dysfunctions
- Post Head Trauma/ Concussion
- Migraine Related Dizziness
- Cervicogenic Dizziness
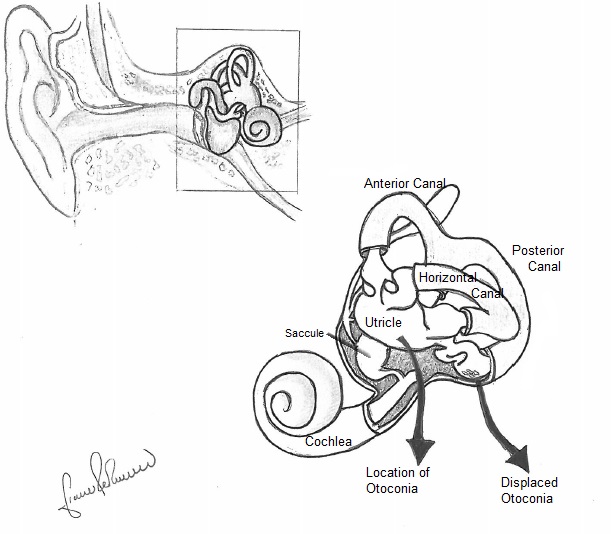 Benign paroxysmal positional vertigo or BPPV is a condition caused by displacement of tiny particles in the inner ear called otoconia. These otoconia are actually calcium carbonate crystals that are normally present in parts of our inner ear called the utricle and saccule which are responsible for informing our brain about where our head is in space relative to gravity. The otoconia are normally held in place on top of a jelly like substance that has a large number of other hair-like structures penetrating into it. A second part of the vestibular system is made up of 3 fluid filled tubes called semicircular canals. As their name indicates they are circular and align in various angles off of the utricle and saccule to sense the direction and speed of our head movements. BPPV occurs when the otoconia break loose from the jelly material in the utricle and make their way into one or more of the semicircular canals. When this occurs there will be certain movements and positions that will result in the feeling of vertigo for a period of time while the otoconia are moving within the canal.
Benign paroxysmal positional vertigo or BPPV is a condition caused by displacement of tiny particles in the inner ear called otoconia. These otoconia are actually calcium carbonate crystals that are normally present in parts of our inner ear called the utricle and saccule which are responsible for informing our brain about where our head is in space relative to gravity. The otoconia are normally held in place on top of a jelly like substance that has a large number of other hair-like structures penetrating into it. A second part of the vestibular system is made up of 3 fluid filled tubes called semicircular canals. As their name indicates they are circular and align in various angles off of the utricle and saccule to sense the direction and speed of our head movements. BPPV occurs when the otoconia break loose from the jelly material in the utricle and make their way into one or more of the semicircular canals. When this occurs there will be certain movements and positions that will result in the feeling of vertigo for a period of time while the otoconia are moving within the canal.
The most common movements that result in the sensation of this type of vertigo are:
- Rolling over in bed
- Looking upward or tilting the head back (such as during hair washing)
- Lying down or getting up from bed
- Bending over (such as during certain yoga poses or to touch ones toes)
- Moving the head quickly
There are many different variations of this condition and the severity can vary from the odd little wave like feeling with certain movements to an inability to move the head at all without losing your lunch. All of which require the movement of the otoconia back to their original position in the utricle in order to relieve the symptoms. It is essential to determine the exact canal that is affected and the type of BPPV that is present in order to successfully treat this condition. A thorough vestibular examination including the use of infrared goggles to examine abnormal eye movements in the dark allows us to determine which ear, which canal and what type of BPPV a person has in order to use the specific maneuvers required to resolve the symptoms of dizziness and imbalance.
This is another set of conditions that may also be referred to as “vertigo” but are altogether different from the BPPV condition described earlier. These conditions are caused by either a bacterial or viral infection of the inner ear itself or the nerve that supplies the vestibular part of your inner ear. This may happen following a bout of illness but can also just hit you out of the blue without warning at all. The primary difference between the labyrinthitis diagnosis and the vestibular neuritis diagnosis is that in the case of the labyrinthitis there is often a loss of hearing that also occurs along with the vertigo symptoms. When these conditions first occur the sensation of spinning can be very intense and many people will be unable to stand or walk without assistance for the first few days. As you can imagine it can be a very scary experience and it often results in a visit to the emergency room due to the intense nausea, vomiting and imbalance that accompanies these conditions. As with any infection the attending Physician will likely treat it accordingly with antibiotics if it is bacterial in nature but if it is a viral infection it is mainly a process of waiting it out just as you would for a cold or flu virus. In many cases the body can fully recover over the course of a few days to weeks but in other cases there can be residual damage to the inner ear or nerve that does not recover fully and a process of neurological adaptation is required.
If there is a degree of damage to the inner ear balance system that remains then the symptoms often change once the initial intense spinning resolves and a person can start to get up and move more again. The degree of symptoms can vary immensely but a few common ones are:
- An inability to focus on an object when the head is moving or a feeling that the eyes drag behind
- Poor tolerance of busy environments such as a grocery store or mall
- Poor tolerance of quick head or body movements
- Blurring of the vision with movement of the head
- Difficulty keeping balanced when walking or veering to one side
- Difficulty keeping balanced in the dark
- Poor tolerance of reading or looking at a computer screen
If a person is experiencing these symptoms it generally indicates that their neurological system is having difficulties compensating for the changes in their balance system caused by the infection. Treatment involving retraining of the nervous system and brain can be very effective in resolving these symptoms and allowing a return to work, sports and life activities that have been limited by the condition. Examination of the specific deficits of the system is required to ensure that the program of retraining is the most effective for each individual as the presentation can vary greatly from person to person.
There is no referral necessary to access our services and there is no wait for our services. Treatment commences on the first appointment date. The assessment typically lasts 45 to 60 minutes. Subsequent treatment sessions are tailored to the individual and last between 15 and 30 minutes.
All sessions are eligible as a form of physiotherapy for coverage through 3rd party health insurance plans.
The TRV Chair is a unique tool for the diagnosis and treatment of benign paroxysmal positional vertigo (BPPV). With the TRV Chair, our expert examiners can rotate their patients 360 degrees along the plane of each semicircular canal. It is also possible to lock the patient in any position for a detailed look at each semicircular canal.

Royal Glenora:
Our Vestibular and Balance Rehabilitation experts in Edmonton are Tayler Gray and Matt Pinard. Tayler heads our Vestibular Program and initially graduated from the University of Alberta in 2001 with Distinction. He holds a Diploma of Advanced Orthopaedic Manual and Manipulative Physiotherapy and is a Fellow of the Canadian Academy of Manipulative PhysiotherapyHe completed post graduate training in vestibular rehabilitation (APTA Vestibular Competency Certification and APTA Advances in Vestibular Rehabiltation Certification) at Emory and Duke Universities respectively.
St. Albert:
Rachel Humphey graduated with a Doctor of Physiotherapy from Bond University, Australia in 2011. She completed post graduate training in vestibular rehabilitation from Emory University and leads our Vestibular North Program.
Windermere:
After graduating from the University of Alberta in 1997, Jonathan Tong has significant experience as a clinical physiotherapist. This experience is bolstered with his extensive post graduate training. He holds a Diploma of Advanced Orthopaedic Manual and Manipulative Physiotherapy and is a Fellow of the Canadian Academy of Manipulative Physiotherapy. He has trained with Tayler Gray and provides vestibular treatment of BPPV at our west location.
Capilano:
Dan Timmermans graduated with a Masters in Physical Therapy from the University of Alberta with distinction in 2009. He went on to complete his post graduate training in Vestibular rehabilitation from Emory University and has APTA Vestibular Competency Certification.
Sherwood Park:
Graham Rayment graduated with a Masters in Physical Therapy from the University of Alberta with distinction in 2010. He went on to complete his post graduate training in Vestibular rehabilitation from Lifemark Institute in 2014 & further accreditation from the American Institute Of Balance vestibular rehabilitation and concussion in 2019. He has trained with Tayler Gray and provides vestibular treatment of BPPV at our Sherwood Park location.
Our vestibular program is robust and not all of our experts are listed here. You can rest assured that our all of our vestibular and dizziness program therapists are continually expanding their treatment skills to provide advanced care and techniques to all our dear patients.
Tayler, Dan, Rachel, Graham, Justin, Adam, Christy and Leading Edge Physiotherapy operate a monthly screening clinic in conjunction with Dr. Allan Ho in the Synergy Wellness Centre in Sherwood Park. Using a multidisciplinary approach we are able to screen for many of the above conditions and triage your condition to ensure the appropriate professional is involved and the most effective treatment is available to you.

Listen: On Vertigo & the TRV Chair With Guest Roberta Slobodian
What's in this Episode? Dizziness is one of the more common complaints among clients that enter the typical medical clinic. It often proves difficult ...
Read MoreEasy Tips to Improve Your Balance – At Any Age
Our balance is something we take for granted. Unfortunately, it is an essential skill for remaining healthy throughout our life. With loss of balance ...
Read MoreMeet our Leading Edge Vestibular Rehabilitation Team in Edmonton, St. Albert & Sherwood Park
At leading Edge Physiotherapy we don't just offer vestibular rehabilitation. We offer a full spectrum of services for those suffering dizziness, balance and vestibular ...
Read MoreDizziness and BPPV
Do you experience any of the following? Bouts of dizziness with changes in head or body positions such as bending down, looking up, rolling ...
Read MoreThe Effects of Repeated Head Trauma and Multiple Concussions
Sidney Crosby was out again - shouldn't we worry about his long term health? Everyone is talking about concussion in sport but there have ...
Read More